MDT: Příběh, který obešel svět
Lidé, místa a okamžiky, které formovaly metodu McKenzie.
Od malého fyzioterapeutického sálu na Novém Zélandu až po ordinaci na všech kontinentech. Objevte, které změnily jednoduchý koncept v globálním hnutí a mnoho příběhů miliony životů.
Tento prostor je věnován sdílení zkušeností, postřehů a inspirativních fyzioterapeutů a dalších odborníků, kteří pracují s mechanickou diagnostikou a terapií (MDT ). Najdete zde kazuistiky, zajímavé klinické momenty i osobní zážitky z praxe, školení a cest. Cílem je propojit kolegy napříč kontinenty, podpořit vzájemné učení a uchovat cenné zkušenosti pro další generaci terapeutů MDT.
Last Tango in Argentina
 It’s over! After 40 years of teaching MDT it is time for me to step aside. My final assignment late last year was a trip to Argentina to present 3 courses. This proved to be the finale of my dreams as I had wonderful students and spectacular patients. So I decided to write an account of my Argentine experiences together with a reflection of my time in the McKenzie world.
It’s over! After 40 years of teaching MDT it is time for me to step aside. My final assignment late last year was a trip to Argentina to present 3 courses. This proved to be the finale of my dreams as I had wonderful students and spectacular patients. So I decided to write an account of my Argentine experiences together with a reflection of my time in the McKenzie world.
Beginnings
In the beginning there was the New Zealand School of Physiotherapy, which heralded the beginning of a run of luck that is unusual even by Las Vegas standards.
1) You have all been through undergraduate programmes and experienced how difficult
it can be to gain entry to physiotherapy or other medical programme. I only had to write a letter and was immediately accepted. Today the only way I could get into a physiotherapy school would be if I was delivering something for Amazon. The same probably applies to Robin, which when you think of it is pretty crazy.
2) I met Robin shortly after graduating when I attended some manual therapy courses
that he was teaching. I spent 2 weeks observing in his clinic and the next day he called
me to ask me to work for him. His assistant had to leave unexpectedly which was my lucky break number two.
3) Those of you who went through the very challenging Probationary Faculty training
programme might want to skip the next two sentences for the sake of your blood pressure. To join the newly formed McKenzie Institute as faculty I was required to fill out a questionnaire. I remember Robin telling me, “It doesn’t matter what answers
you give, you are in”.
4) After I had been teaching for about 5 years, MII developed the Diploma Programme and my colleagues and I were all grandfathered in. When I think of the effort it takes
to get the Diploma now I do feel a little sheepish.
Timing it would seem is everything.
Early Years Teaching
The contrast with our education programme when I began and now could not be greater. Robin’s idea of preparing new faculty, and back then we were all new, was to have us attend
a couple of courses observing him and becoming familiar with the slides. After this, armed
When I started teaching in the early 80’s, there was no Part A-D; just a single 4 day course on the lumbar spine where Robin would see at least 12 patients. On the last day he would sometimes pull someone out of the audience to demonstrate how the same principles could be applied to a neck problem. To him it was so obvious that he assumed everyone would be able to copy his approach. I did copy it; I copied it in the same way that a parrot will imitate the human voice and my teaching was probably as effective as those lovable birds. The students struggling through 12 patient demonstrations, during which I desperately hoped that some of them would get better.
As our faculty grew we began to produce our own course manuals. There was no standardisation and how and what was taught was often at the whim of the instructor. There was a standard slide package but not all faculty used it. It wasn’t until Helen Clare became in charge of education that things immediately began to improve. Happily this improvement has continued and today we have an educational product that we can be proud of.
Argentina
Now let’s head back to Argentina and see how my story ends. If you had to choose a place to present your last courses Buenos Aires would be at or near the top of the list. The city is beautiful, the people are warm and friendly and there is a small, dedicated group who pitch in to organise the courses. Unfortunately, like several of our branches, they struggle to fill the courses. Despite energetic marketing the numbers for the part A and C were low, just 10 and
8 respectively, but despite this the courses were highly successful. All the students on the Part A had been taught at the under graduate level by two of the Argentine Board members who had given them an excellent introduction to MDT. What they were also able to do was to fill them with an enthusiasm for MDT and clinical reasoning. This again emphasises the importance of having MDT properly taught at under graduate level.
Looking back I’m not sure if I had previously identified a case like this where a
standard lateral shift, responding to side glide and extension, quickly became a flexion responder with a significant lateral component, especially after he spent several hours supposedly in prolonged flexion.
The other satisfying feature of this case was the wonderful teaching opportunity to be able to demonstrate such dramatic changes in obstruction when the correct movement was identified.
2) This patient was a professional dancer and she was complaining of a hip problem. This seemed less likely when she indicated that her pain was posterior thigh; another
good teaching moment. It had been present for 5 years and was unchanging. She described difficulty in jumping, in the type of move which ballerinas do when they appear to be doing the splits as they fly though the air. “When I lead with my left leg on a jump the height is considerably lower than when I lead with my right leg” she explained.
Her other functional difficulty really got my attention. She told me that she could not put her left heel behind her head when she was sitting. As soon as she said this I knew that I was making the correct decision in retiring from teaching. It was a shock to realise, perhaps for the first time, that I could not do this either. Time had clearly
taken its toll on my body and retirement seemed my only option.
She had a slight loss of flexion and external rotation in her left hip and painless weakness of hip abduction. Time to test the spine. As you can imagine a professional dancer will have a very flexible spine and my patient was no exception. However after doing a series of EIL exercises with overpressure applied to her mid lumbar
spine up to lower thoracic, all her movements and functional tests became normal. She was sent home to do EIL with belt fixation and returned the next day symptom free with full function. She also said that she had taken a ballet session after our treatment and for the first time in 5 years her dance positions felt normal. To say the least, she was thrilled and asked the translator if it was okay to hug me. Naturally I gave this request serious consideration before agreeing.
In conclusion I will say that there are few days that go by when I do not give silent thanks to the members of the EXPOSS team for the great job they did drawing our attention to how necessary it is to truly clear the spine when managing an extremity problem.
3) This patient was a woman in her mid-40’s who was a passionate runner. 20 years
earlier she had dislocated her patella during a kick boxing session. She had experienced occasional dislocations since then but they were occurring much more frequently in the last 3 months. She said that some days the patella might dislocate up to 6 times with minimal provocation. On other days she could run through rough hill country trails without any problem. This was another big teaching moment. My wife of 46 years has experienced patella subluxation and dislocation throughout her life
and so I’m familiar with how disabling this can be. The seemingly random nature of
my patient’s incidents struck me as atypical: often able to run hard on hilly terrain without symptoms and other times subluxing when walking across the room.
The surgeon she saw told her very bluntly to stop running and that she needed surgery. This upset her a great deal as running was a major part of her life. She did around 60 km a week, often over rough hilly trails.
On examination she had a slight loss of knee flexion and pain on resisted extension. There was tenderness and paraesthesia around the medial aspect of her patella
(another clue from Exposs). Stairs were painful and she was unable to fully squat. She had no history of back pain, but as you might guess EIL overpressure and extension mobilisation took away all her symptoms and she could squat normally.
At follow up the next day she reported being pain free with no dislocations, despite a strenuous hill run. When I asked her if she intended to see the surgeon again her face contorted in anger. “No” she snarled!!
We monitored her progress over the next week and she remained symptom free. Early in February, this year, I received an email from the patient’s sister-in-law, who was a participant on the course. She was pleased to tell me that her sister-in-law has remined symptoms free. I’m not sure how many of you may have had patients with apparent subluxations that responded to spinal loading, but I recall another patient with a similar response. This was a teenage boy who was an elite hockey player. He reported that he felt his shoulder sublux downwards if another player pulled on his stick. I tested this and with 1 hand on his shoulder I could feel a very pronounced and abnormal caudal slide of
the humerus. After repeated extension movements of his cervical and upper thoracic spine his shoulder was completely stable to this type of force.
I don’t have an explanation for these phenomena and would be interested to know if others have found the same thing, but it does demonstrate the unexpected response
that can occur with therapeutic loading.
I’m not sure how many of you may have had patients with apparent subluxations that responded to spinal loading, but I recall another patient with a similar response. This was a teenage boy who was an elite hockey player. He reported that he felt his shoulder sublux downwards if another player pulled on his stick. I tested this and with 1 hand on his shoulder I could feel a very pronounced and abnormal caudal slide of
the humerus. After repeated extension movements of his cervical and upper thoracic spine his shoulder was completely stable to this type of force.
I don’t have an explanation for these phenomena and would be interested to know if others have found the same thing, but it does demonstrate the unexpected response
that can occur with therapeutic loading.
4) Another dancer and another apparent hip problem. This time the pain was in a more typical location at a precise point in the R groin. It had been present for 13 years and the patient explained that she always danced with pain and it had become so
distressing that she was seriously considering retirement. She said that she was worse when she landed from a jump, especially if her hip was flexed, worse when she sat
and when she went up stairs. On examination there was a 25 degree loss of hip flexion and also internal rotation loss. Resisted movements were painless. Trunk rotation was limited to the left. The functional test was a 1 leg squat and stepping up with her right leg.
She said that the only thing which gave her some relief was extension exercises of her spine.
I’m sure that you will guess the rest. EIL overpressure throughout the lumbar and thoracic spine and extension mobilisation substantially reduced her pain to an extent she had not experienced in 13 years.
As you can imagine, a professional female dancer will present with an excellent range of motion, including spinal extension, and watching her extend there was no
indication of restriction. Also, both dancers regularly did extension stretches as part of their training, but clearly that was not enough to prevent some sort of spinal influence on their lower extremity symptoms. In addition neither had any complaint of back
pain, but after small movement increases at specific levels their symptoms abolished
or greatly diminished. Again I have no explanation but can only wonder at the mysteries of our bodies. Clearly this is an area that needs further investigation.
Anyone willing to take it on?
5) At last an extremity that was an extremity! This was a 2 month long ankle pain that occurred during a basketball game when the patient landed from a jump in a position
of plantar flexion and eversion. At the time of his assessment he was not responding
to self-treatment exercise. Squatting and forced eversion were painful but the patient could run and jump with no symptoms. On examination there was a significant loss of dorsiflexion with only minimal loss in other directions. Resisted movements were not painful. His functional test was squatting which was clearly limited.
With the injury occurring in plantar flexion and a major loss of dorsiflexion it would be reasonable to suspect that if a derangement was present the directional preference would be dorsiflexion and this is what the group predicted. The opposite was in fact the case. Repeat plantar flexion in kneeling rapidly improved his functional test and eventually he became symptom free as he continued pushing to end range. As a bonus we were able to re derange his ankle with repeated dorsiflexion.
These patients were certainly interesting and provided wonderful teaching moments, but they were not particularly difficult and I’m sure that anyone reading this account would have got similar results. However they do illustrate the power of MDT to
classify and identify the appropriate course of management. The majority of the cases were chronic, some of several years duration and they had failed other conservative care, so for me it was a reminder of what a wonderful system we have had entrusted
to us.
First I want to thank the Argentine Branch for making my final teaching courses so memorable. Their friendship, warmth and generosity will be something I will always remember.
When I began teaching 40 years ago I had no idea that I was about to embark on the most incredible ride. Teaching MDT around the world has been a privilege for which
I am very grateful and my experiences in Argentina have reinforced that feeling. How fortunate we are to work in an area where there is so much more to explore and
uncover. Many years ago I recall Robin saying, “We have only scratched the surface when it comes to MDT”. How right he was.
He also said that we are here for the patient. Looking back over 40 years of teaching, the highlights have been the patients I have seen on courses in different parts of the world.
One of the great strengths of the McKenzie educational programmes is that we see actual patients during the courses. This is not only a wonderful teaching tool but it
also gives the system immediate credibility in the eyes of the participants. We have added a lot of material on drivers of pain and how to manage them, but when we assess a patient in front of the participants they see how pain drivers are managed in a real situation. Role play and case studies have their place but nothing can replace live patient demonstrations. That said I am glad that we are no longer seeing 12 on a Part A.
Advise to new teachers:
1)Develop your own style of teaching, something that is comfortable for you. Years
ago MII adopted the policy of trying to provide different instructors during A-D, so that participants would be exposed to a variety of styles. I believe that this policy strengthens our educational programme.
2)When I started teaching Robin gave me one piece of advice.
“If you make a mistake admit it and don’t try to cover it up. Whenever I’ve tried to deny making a mistake it hasn’t worked and I end up looking worse than if I’d accepted my error”.
I’ve followed his advice and found that people usually appreciate your honesty and the issue dies right there.
3)Regarding the issue of assessing patients in front of a group, I used to find this
very stressful because I felt a pressure within me that I had to get the patient better
otherwise I would lose all credibility. It was not until I did some work with
Charles Aprill that I realised that I was missing the most important part of MDT, which is to concentrate on assessing. If someone gets better that is a bonus, but the main point is to demonstrate the MDT assessment process. Interestingly when I started following this approach to patient care my clinical results improved significantly.
I am very grateful for all the help I have received in my career and the many friends I have made. We are fortunate to be in a profession with such enormous potential for improving the lives of our fellow humans and in this turbulent world that is a comforting thought.
ČJ
Poslední tango v Argentině
Colin Davies (předseda McKenzie Institutu International)
Překlad Eva Nováková
Je konec! Po 40 letech výuky MDT nastal čas, abych ukončil svou kariéru instruktora MDT. Mým posledním úkolem na konci loňského roku byla cesta do Argentiny, kde jsem přednášel na třech kurzech. Ukázalo se, že to bylo finále mých snů, protože jsem měl úžasné studenty a velkolepé pacienty. Proto jsem se rozhodl napsat zprávu o svých argentinských zážitcích spolu s reflexí mého působení v McKenzie světě.
Počátek
Na začátku byla novozélandská škola fyzioterapie, která předznamenala začátek běhu za štěstím, který je neobvyklý i na poměry Las Vegas.
1) Všichni jste prošli bakalářskými programy a zažili jste, jak obtížné je dostat se na fyzioterapii nebo jiný lékařský program. Mně stačilo napsat dopis a byl jsem okamžitě přijat. Dnes bych se na fyzioterapeutickou školu dostal jedině tehdy, kdybych rozvážel něco pro Amazon. Totéž pravděpodobně platí i pro Robina, což je, když se nad tím zamyslíte, dost šílené.
2) S Robinem jsem se seznámil krátce po ukončení studia, když jsem navštěvoval kurzy manuální terapie, které Robin vyučoval. Strávil jsem dva týdny pozorováním na jeho klinice a následně mi Robin zavolal a požádal mne, abych pro něj pracoval. Jeho asistentka musela nečekaně odejít, což bylo moje štěstí číslo dvě.
3) Ti z vás, kteří prošli velmi náročným MDT školením fakulty na pozici instruktora, budou možná chtít přeskočit moje následující dvě věty a to kvůli zvýšení krevního tlaku. Abych mohl nastoupit do nově vzniklého McKenzieho institutu jako pracovník fakulty, musel jsem vyplnit dotazník. Vzpomínám si, jak mi Robin řekl: „Nezáleží na tom, jaké odpovědi napíšeš, jsi přijat“.
4) Poté, co jsem učil asi pět let, MII vyvinul Diplomovaný program a všichni moji kolegové a já jsme byli zařazeni do programu senior instruktorů. Když si vzpomenu na úsilí, které je třeba vynaložit k získání diplomu nyní, připadám si tak trochu jako ovce.
Správné načasování je to, na čem vše stojí.
První roky výuky
Náš vzdělávací program měl oproti současnému vzdělávání značné odlišnosti. Robinova představa o přípravě nových učitelů, a tehdy jsme byli všichni noví, spočívala v tom, že nás nechal navštěvovat pár kurzů, kde jsme ho pozorovali a seznámili se s diapozitivy. Poté jsme se vyzbrojeni starými kopiemi Robinových diapozitivů vydali na vlastní pěst do výuky.
Když jsem na začátku 80.let začínal učit, neexistovala žádná část A-D; pouze jediný čtyřdenní kurz bederní páteře, kde Robin vyšetřoval nejméně 12 pacientů. Poslední den si občas někoho vytáhl z publika, aby mu předvedl, jak lze stejné principy aplikovat na problém s krční páteří. Pro něj to bylo tak samozřejmé, že předpokládal, že každý bude schopen jeho přístup okopírovat. Já jsem ho kopíroval; kopíroval jsem ho stejným způsobem, jakým papoušek napodobí lidský hlas, a moje výuka byla pravděpodobně stejně účinná jako zpěv milých papoušků. Studenti se trápili s demonstracemi dvanácti pacientů, během nichž jsem zoufale doufal, že se mi některý z pacientů zlepší.
Jak se naše fakulta rozrůstala, začali jsme vytvářet vlastní příručky pro kurzy. Neexistovala žádná standardizace, a to, jak a co se učilo, bylo často na libovůli instruktora. Existoval standardní balík diapozitivů, ale ne všichni vyučující ho používali. Teprve v momentě, kdy se Helen Clare (nyní na pozici předsedkyně správní rady MII) stala vedoucí vzdělávání, situace se okamžitě začala zlepšovat. Naštěstí toto zlepšování pokračovalo a v současnosti máme vzdělávací produkt, na který můžeme být hrdí.
Argentina
Nyní se vraťme do Argentiny a podívejme se, jak můj příběh končí. Kdybyste si měli vybrat místo pro prezentaci svých posledních kurzů, Buenos Aires by bylo na prvním místě seznamu. Město je krásné, lidé jsou vřelí a přátelští a existuje zde malá, obětavá skupina, která se podílí na organizaci kurzů. Bohužel, stejně jako několik našich poboček MII, mají problém kurzy naplnit. Navzdory energickému marketingu byl počet účastníků na částech A a jednoho C nízký, jen 10, 10 a 8 účastníků, ale přesto byly kurzy velmi úspěšné. Všichni studenti, kteří se účastnili části A, se již dříve učili na vysoké škole od dvou argentinských členů McK Institutu Argentina a od nich měli vynikající úvod do MDT. Kolegové je dokázali naplnit nadšením pro MDT a klinické uvažování. To podtrhuje důležitost řádné výuky MDT na úrovni vysokoškolských studentů.
Pacienti:
- U prvního pacienta došlo před několika dny k vybočení, u kterého byla zpočátku dobrá reakce na autoterapii korekcí lateroposunu a extenzi. Nicméně po dlouhé cestě na zadním sedadle malého auta se příznaky a stav pacienta změnil a na extenzi již nereagoval. Jeho bolest byla do pravé hýždě a vybočení bylo kontralaterální. Došlo k výrazné ztrátě flexe a lateroposunu doprava. Opakovaný stoj ve flexi příznaky zhoršil a opakovaný stoj v extenzi neměl vliv na symptomy, ale následně se zhoršil jeho rozsah do flexe, zatímco extenze se zlepšila. Opakovaný lateroposun doprava nezhoršil příznaky a zlepšil rozsah lateroposunu. Proto toto dostal za domácí cvičení.
Následující den došlo k malému zlepšení jak jeho příznaků, tak rozsahu pohybu ve flexi a lateroposunu. Protože příznaky byly proximální, neprovedl jsem během prvního dne žádné neurologické testování, protože pacient si na kvalitu chůze nestěžoval. Otestoval jsem tedy opožděně Lasegue a zjistil jsem, že Lasegue vpravo reprodukuje jeho bolest do hýždě při 60 stupních a Lasegue vlevo při 70 stupních. Když se ohlédnu zpět, pravděpodobně jsem v minulosti nedostatečně používal napínací manévry jako základní baseline. Jeho flexe byla stále velmi omezená a měl deviaci doleva. V reakci na opakovanou flexi vstoje na stupínku, abych srovnal deviaci se jeho rozsah flexe zlepšil a všechny příznaky se rychle odstranily a tento efekt přetrvával.
Když se ohlédnu zpět, nejsem si jistý, jestli jsem už dříve zažil podobný případ, kdy při standardní korekci vybočení, reagující na lateroposun a extenzi, se vše tak rychle změnilo ve flexi s výraznou laterální komponentou, zejména poté, co strávil údajně několik hodin v setrvalé flexi na zadním sedadle auta.
Dalším benefitem této kazuistiky byla úžasná výuková příležitost, kdy bylo možné demonstrovat dramatické změny odstranění blokády při identifikaci správného pohybu.
- Tato pacientka byla profesionální tanečnice a stěžovala si na problémy s kyčlemi. Tato oblast se přestala jevit jako zásadní, jakmile uvedla, že její bolest se přesouvá do zadní strany stehna – to byl další dobrý moment pro výuku. Obtíže měla již 5 let a bolest byla neměnná. Popisovala potíže při skocích, při pohybech, které dělají baletky, při roznožkách, když letí vzduchem. „Když při skoku vedu levou nohu, výška je podstatně nižší, než když vedu pravou,“ vysvětlovala.
Její další funkční limitace mě opravdu zaujala. Sdělila mi, že si při sedu nemůže dát levou patu za hlavu. Jakmile mi toto sdělila, věděl jsem, že jsem se rozhodl správně ukončit výuku a již nebýt lektorem
Sinikka Kilpikoski: A Life Shaped by Hands, Curiosity, and Lakeside Saunas
 Hi, I’m Sinikka Kilpikoski. My journey as a physiotherapist began way back in 1969 when I graduated in the city of Tampere, Finland. Not long after, I packed up and moved to a tiny village tucked in the heart of Finland, where I opened a small private clinic—just me and my treatment table. But my hunger to learn never left.
Hi, I’m Sinikka Kilpikoski. My journey as a physiotherapist began way back in 1969 when I graduated in the city of Tampere, Finland. Not long after, I packed up and moved to a tiny village tucked in the heart of Finland, where I opened a small private clinic—just me and my treatment table. But my hunger to learn never left.
Soon, I found myself diving deep into the world of manual therapy. Norwegian instructors traveled to Finland to teach us the principles of Orthopaedic Manual Therapy (OMT). We studied extremities (Part E) and the spine (Part C), learning techniques from the likes of Freddy Kaltenborn, Olaf Evjenth, and Hans Gunnari. Alongside them, Odvar Holten and Rolf Gustafssen introduced us to training therapy—something revolutionary in Finland at the time. As if that weren’t enough, I also had the privilege of learning from the legendary Professor Vladimir Janda from Czechoslovakia, who opened our eyes to the concept of muscle imbalance.
In 1986, I returned to school to specialize in Public Health and Geriatric Physiotherapy at the Applied University of Jyväskylä. After that, I wasn’t quite done. I enrolled at the University of Jyväskylä’s Department of Health Sciences and graduated in 1994 with a Master of Health Sciences. Somewhere in the middle of that academic whirlwind—in 1988—I took a course with a man named Robin McKenzie in Helsinki. That course lit a fire in me. I had found my path: Mechanical Diagnosis and Therapy (MDT).
From there, the MDT journey unfolded quickly. I attended Part B and C courses in Helsinki with Malcolm Robinson (UK) and Mark Laslett (New Zealand), and Part D in Newcastle upon Tyne, England, taught by the unforgettable Ace Neame (NZ). It was there I heard whispers about MDT conferences and the possibility of becoming a Diploma holder. So, off I went to my first international MDT Conference in Dallas, Texas—what a leap! I applied to the Diploma program, packed my bags, and in early 1993, I flew to New Zealand. My English wasn’t perfect, but I passed both the Credentialing and Diploma exams that April. I’m proud to say I’m MDT Diploma holder #56.
Before teaching in Finland, I had the chance to co-instruct alongside my mentor Riki Yamada from Canada, who came to Finland to help introduce the A and B parts of the course. Later, I spent valuable time with her and other generous MDT instructors—Phil Burchell and Colin Davis—in places like Montreal, London (Ontario), Thunder Bay, and Ottawa. Their support was truly formative. I consider myself incredibly lucky to have been guided by such exceptional clinicians.
In 1995, I officially began teaching MDT courses in Finland and decided to take my studies one step further: a PhD. My dissertation, “The McKenzie Method in Assessing, Classifying and Treating Non-Specific Low Back Pain in Adults with Specific References to the Centralization Phenomenon,” was publicly defended in December 2010. It included five original published articles.
Throughout all these years, I’ve remained rooted in clinical practice. My clinic—Vaajakosken Kuntohoito Oy—will celebrate its 50th anniversary in May 2026! I started solo in 1976, and now the clinic is in the capable hands of my youngest son, also a physiotherapist and now our CEO. We’re a team of eight physios and one masseur. Every physiotherapist on our team is MDT-credentialed, and our clinic is still the only internationally certified McKenzie clinic in Finland.
I’ve served as a Senior Instructor with the McKenzie Institute International (MII), primarily teaching Parts C, D, and Advanced E courses—all in Finnish, of course. I’ve also been responsible for organizing Credentialing Exams here in Finland.
Since earning my PhD, I’ve worked as a postdoctoral researcher in the Department of Physical Medicine and Rehabilitation at the Central Hospital in Jyväskylä. I’ve been fortunate to co-author some original articles, including:
- “Comparison of magnetic resonance imaging findings among sciatica patients classified as centralizers or non-centralizers,”
- and “The McKenzie Method versus guideline-based advice in the treatment of sciatica: 24-month outcomes of a randomized clinical trial.”
Up next, we’re preparing a secondary analysis from that same study. This upcoming paper looks at the direct healthcare costs and number of sick leave days over a 24-month period. Spoiler: both groups—McKenzie and guideline-based advice—showed significant clinical improvements in pain and disability, with no major difference between them. Discectomy rates were also similar. Our new analysis, titled “Economic Evaluation of Costs in Sciatica Patients Treated by the McKenzie Method or Guideline-Based Advice,” is headed for English screening next week and then off to Clinical Rehabilitation (SAGE Journals). Fingers crossed!
Since that first MII Conference in Dallas, I’ve attended every single international MII Conference, nearly every European MDT Meeting since 1992, and even a few North American ones. Whether the Alicante conference was my last? Who knows—perhaps the lakes and saunas are calling louder now.
Speaking of which… I still treat patients at my clinic, but come summer, my husband and I escape to our lakeside cottage, just five kilometers from our winter home and the clinic. That’s when life truly bursts to the brim: our three adult children, their partners, and our seven grandchildren (aged 10 to 22) fill the house. There’s laughter, sauna, swimming, fishing, and the pure, joyous chaos of multigenerational summers by the lake.
With warm regards,
Sinikka Kilpikoski
ČJ
Sinikka Kilpikoski: Život mezi pacienty, metodou McKenzie a letními saunami
Jmenuji se Sinikka Kilpikoski a moje cesta fyzioterapeutky začala v roce 1969 v Tampere, ve Finsku. Krátce nato jsem se přestěhovala do malé vesničky v srdci Finska, kde jsem si otevřela soukromou praxi – jen já a mé ruce. Ale chuť učit se dál mě nikdy neopustila.
Začala jsem tedy navštěvovat různé manuální kurzy – části E (periferní klouby) a C (páteř). Do Finska tehdy jezdili norští fyzioterapeuti, aby nás seznámili s principy ortopedické manuální terapie podle Freddyho Kaltenborna, Olafa Evjentha a Hanse Gunnariho. A nejen to – Odvar Holten a Rolf Gustafssen nás učili základy tréninkové terapie, což byla tehdy ve Finsku naprostá novinka. A jako třešničku na dortu jsem měla možnost učit se v Helsinkách od profesora Wladimira Jandy z Československa, který nás zasvětil do konceptu svalových dysbalancí.
V roce 1986 jsem se rozhodla vrátit do školních lavic a specializovala jsem ve fyzioterapii veřejného zdraví a geriatrie na univerzitě v Jyväskyle (Univerzita aplikovaných věd). A protože jsem se do učení zamilovala, pokračovala jsem dál – na Univerzitě v Jyväskyle jsem vystudovala magisterský obor Zdravotní vědy. Během tohoto studia jsem přemýšlela, čemu bych se chtěla jako lektorka věnovat. A pak přišel rok 1988 a s ním kurz Part A v Helsinkách s Robinem McKenziem. A bylo rozhodnuto – vydávám se cestou MDT.
Následovaly další kurzy: části B a C jsem absolvovala v Helsinkách pod vedením Malcolma Robinsona (Velká Británie) a Marka Lasletta (Nový Zéland). Part D jsem navštívila v anglickém Newcastlu, kde nás učil Ace Neame z Nového Zélandu. Právě tam jsem se dozvěděla o mezinárodních konferencích McKenzie institutu (MII). Vydala jsem se tedy na svou první – do Dallasu v Texasu. A tam jsem zjistila, že se MDT dá studovat až k diplomu… v Novém Zélandu. Tak jsem se přihlásila a v roce 1993 jsem odletěla na druhý konec světa. Přestože moje angličtina nebyla zrovna výstavní, zvládla jsem jak credentialing, tak i diplomovou zkoušku – a stala jsem se držitelkou diplomu číslo 56.
Než jsem začala kurzy vyučovat doma ve Finsku, měla jsem obrovské štěstí – přijela za mnou moje mentorka Riki Yamada z Kanady, se kterou jsem mohla spolulektorovat části A a B. Poté jsem strávila čas s ní, s Philem Burchellem a s Colinem Davisem – na kurzech v Montrealu, Londýně (Ontario), Thunder Bay a Ottawě. Tito kolegové mě podpořili, věnovali mi svůj čas, nechali mě učit s nimi. Dodnes jsem za tuhle zkušenost nesmírně vděčná.
V dubnu 1995 jsem začala oficiálně vyučovat kurzy MDT ve Finsku – a zároveň jsem se rozhodla pokračovat i ve výzkumu. Začala jsem připravovat doktorskou práci na Univerzitě v Jyväskyle. Její název?
„Metoda McKenzie při hodnocení, klasifikaci a léčbě nespecifických bolestí dolní části zad u dospělých s důrazem na fenomén centralizace.“
Disertaci jsem obhájila veřejně 3. prosince 2010. Zahrnovala pět původních článků publikovaných v odborných časopisech.
Celou tu dobu jsem ale zůstala věrná klinické praxi. Moje soukromá klinika Vaajakosken Kuntohoito Oy oslaví v květnu 2026 úctyhodných 50 let! Začínala jsem sama, ale dnes pracujeme v týmu osmi fyzioterapeutů a jednoho odborného maséra. Všichni fyzioterapeuti mají složený credentialing a naše klinika je stále jedinou mezinárodně certifikovanou McKenzie klinikou ve Finsku. A co víc – vedení teď převzal můj nejmladší syn, který je také fyzioterapeutem a dnes i CEO.
V rámci McKenzie institutu jsem dosud aktivní jako Senior Instructor a vyučuji především části C, D, pokročilé kurzy E a opakovací kurzy – všechny samozřejmě ve finštině. Také se podílím na organizaci credentialingových zkoušek u nás.
Po dokončení doktorátu jsem začala působit jako postdoktorandka v Centrální nemocnici ve Finsku, na oddělení fyzikální medicíny a rehabilitace. Měla jsem možnost spolupracovat na několika výzkumech. Například:
- „Porovnání nálezů magnetické rezonance u pacientů s ischiasem klasifikovaných jako centralizující nebo necentralizující“,
- a „Metoda McKenzie vs. doporučení dle klinických směrnic u léčby ischiasu: 24měsíční výsledky RCT studie“.
A teď chystáme sekundární analýzu z téže studie.
Malý spoiler: Obě skupiny (McKenzie i skupina dle směrnic) se klinicky i statisticky zlepšily v bolesti a disabilitě – bez zásadního rozdílu. Ani počty operací (diskektomií) se nelišily.
Proto se chystáme publikovat analýzu přímých nákladů na zdravotní péči a pracovní neschopnosti v průběhu dvou let. Článek ponese název:
„Ekonomické hodnocení nákladů u pacientů s ischiasem léčených metodou McKenzie nebo podle klinických směrnic: sekundární analýza RCT“
Příští týden jde text na jazykovou korekturu do angličtiny a pak směřuje do časopisu Clinical Rehabilitation (SAGE Journals). Věříme, že zaujme!
Od prvního setkání s MII konferencí v Dallasu jsem se zúčastnila všech mezinárodních MII konferencí, téměř každého evropského MDT setkání od roku 1992 a pár severoamerických. Jestli byla Alicante poslední? Kdo ví. Možná už volá finské jezero…
A ano – stále aktivně pracuji s pacienty. V létě se s manželem stěhujeme na chatu u jezera, pět kilometrů od zimního domova a kliniky. A tam to žije! Tři dospělé děti, jejich partneři, sedm vnoučat ve věku 10–22 let a jejich kamarádi. Všichni se sjíždějí kvůli sauně, koupání, rybaření a hlavně – být spolu.
S přáním všeho dobrého,
Sinikka Kilpikoski
Memories of a Unique Gathering
By George Spanos
The Decision to Host in Greece
 It was in June 1998 when we, at the Greek branch of the McKenzie Institute, decided to organize that year’s Euromeeting in Paros.
It was in June 1998 when we, at the Greek branch of the McKenzie Institute, decided to organize that year’s Euromeeting in Paros.
From the previous year, all European branches had expressed a strong wish that Greece should host the next meeting. We accepted the challenge with joy — but under two conditions.
First, the hospitality would take place on an island. Not in Athens, but in a true Greek island setting.
Second, no one should come all the way to Greece — and especially to its islands — for just a single day, as usual. The event would therefore last at least two days. And so it did.
This Euromeeting proved to be unique for many reasons. It was the only two-day event ever held. The setting was magical — the island of Paros, one of the most beautiful in Greece. The organization was meticulous, with surprises and events far beyond expectations. And perhaps most importantly, the gathering was graced by the presence of Joy and Robin McKenzie themselves — something unprecedented in those times.
This narrative is dedicated to the memory of Robin McKenzie and to the menory of Professor of Orthopaedic Medicine Apostolos Polyzoidis, pioneer in knee prosthetics, advisor to the Greek branch, and my close friend. It is also dedicated to my best man and woman, Dimitris Pt cred MDT and Thalia Sifneos that they gave their heart to the organization, to all my colleagues that came from across Europe, and especially to Sara Luetchford and Antoine Gemayel — the only two from those years who are not yet retired, and fortunately still well and active today.
Arrival of the McKenzie Family
I will never forget that summer morning in June 1998. My little Fiat Uno Turbo seemed like an airplane as I rushed along the narrow island roads to the small Paros airport, where Robin and Joy were arriving.
I worried the car would be too small for their luggage and wondered if I could find a taxi if needed. By the time I arrived, their twin-engine plane had already landed. They stood smiling outside the tiny terminal, waiting.
After warm greetings, I asked anxiously if I was late.
“No,” they laughed, “we just arrived.” Already, they were enchanted by the island.
I loaded the luggage into the car, and as we drove towards Naousa Bay, both Robin and Joy expressed their excitement.
“It reminds us so much of New Zealand,” they said together.
“Yes,” I answered, “we want you to feel at home — both in the environment and in spirit.”
The Bay of Naousa and the Destroyer Themistocles
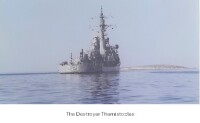 About forty-five minutes later, we arrived at the beautiful Porto Paros Hotel, overlooking Naousa Bay. Across the water lay the dazzling white town of Naousa, like a painting in blue and white, its harbor filled with small fishing boats.
About forty-five minutes later, we arrived at the beautiful Porto Paros Hotel, overlooking Naousa Bay. Across the water lay the dazzling white town of Naousa, like a painting in blue and white, its harbor filled with small fishing boats.
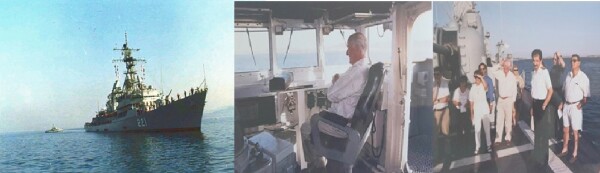
Only one sight stood in stark contrast — a gray destroyer, the HS Themistocles of the Hellenic Navy, anchored in the bay. None of us knew yet the role this ship would play in the story of the Euromeeting.
An Unexpected Patient
That afternoon, while preparing the conference hall, I was called urgently by the hotel director, Mr. George Malepitzopoulos. He explained that the commander of the destroyer, Captain Vasilis Tsitonakis, had been bedridden for a week with severe lumbar sciatica unable to perform his duties.
I visited him immediately. He presented with serious scoliotic and kyphotic deformity, radiating pain below the knee, and neurological deficits despite strong medication. After examination, I performed manual correction of his lateral shift. Within minutes, his pain centralized diminished, and his trunk straightened.
He was astonished. “Unbelievable! I feel so much better. What do I owe you?”
“Nothing,” I said. “Do your exercises faithfully and I’ll see you tomorrow.”
Opening of the Euromeeting
 The next morning the Euromeeting began. The atmosphere was festive, as old friends and colleagues reunited. I chaired the session, with the late Ann Robinson, wife of Malcolm Robinson from the UK branch, as secretary.
The next morning the Euromeeting began. The atmosphere was festive, as old friends and colleagues reunited. I chaired the session, with the late Ann Robinson, wife of Malcolm Robinson from the UK branch, as secretary.
During the first break, I visited Captain Tsitonakis. He was radiant, enjoying breakfast.
“I feel wonderful! Thank you. Please, tell me how I can repay you.”
At first I refused, but then I suggested: “We are hosting the European meeting of the International McKenzie Institute, with the founder Robin McKenzie himself present. Could you honor him — and us — by inviting the delegates for a guided visit on board your ship?”
“Of course!” he replied. “It would be my honor. Come at 6 p.m. today.”
I returned to the hotel and left a note for the delegates: “If you wish to experience a pleasant surprise, gather at the hotel beach this afternoon. Dress code: casual. Don’t miss it!”
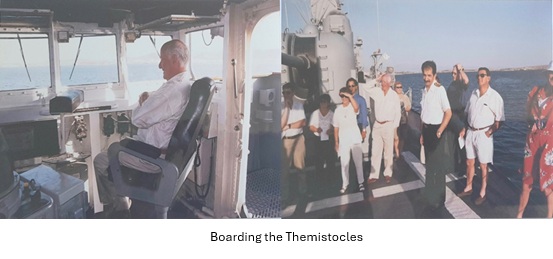
Boarding the Themistocles
 In the afternoon, we gathered at the beach, all guessing what the surprise could be. A navy launch approached, and we boarded. As we drew near the destroyer, excitement rose.
In the afternoon, we gathered at the beach, all guessing what the surprise could be. A navy launch approached, and we boarded. As we drew near the destroyer, excitement rose.
Suddenly, the ship’s crew appeared on deck, in full dress uniform. A ladder was lowered. The commander ordered a military salute. One by one, we were welcomed aboard — Robin and Joy first, then all the delegates.
We toured the ship: communication systems, radars, missiles, torpedoes, depth charges. Robin was even invited to the bridge and seated in the captain’s chair.
At the end, Captain Tsitonakis invited us to a banquet aboard — an unforgettable meal of naval hospitality.
When we returned to shore, excitement was overwhelming. The meeting had already exceeded all expectations.
Nights of Celebration
That evening, by the hotel pool, the director Mr Malepitzopulos hosted a splendid Cycladic night — local dishes, fine Parian wine, and traditional island dances. Under the full moon rising over Naousa Bay, colleagues laughed, danced, and celebrated late into the night.
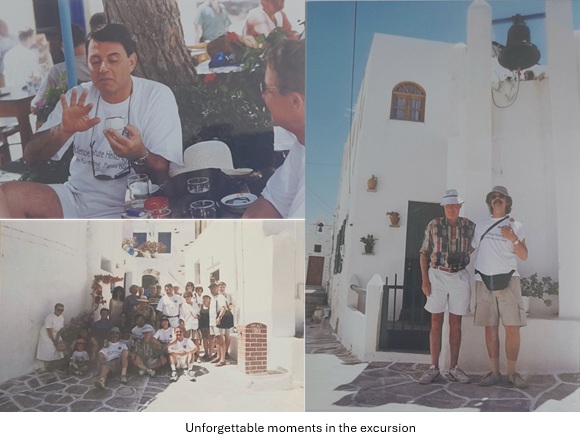
Excursions and Lectures
The following morning began with an excursion to the ancient marble quarries at Marathi. Later that day, Professor Apostolos Polyzoidis gave a lecture on the famous Parian marble — translucent, dazzlingly white, the stone from which the Athens Acropolis and Erechtheion with its Caryatids were built. He also spoke about the prehistoric Cycladic civilization.
The lecture took place in the historic Church of Panagia Ekatontapyliani, founded in 237 AD and expanded by Emperor Justinian in the 6th century, inspired by Hagia Sophia. It was a magnificent setting for such a lecture.
Later, we wandered through the village streets of Lefkes lined with bougainvillea and hibiscus. Two memories stand out: Robin and I ringing the bell of a small church together, and Antoine Gemayel reading Margarita’s fortune in her coffee at the local café — to everyone’s delight.
A Private Concert
That evening, Professor Polyzoidis invited all participants to his villa. After a lavish dinner under the starlit Parian sky, the highlight came: the renowned soprano Cathrin Monès, guest of the professor, gave a moving recital in honor of the Euromeeting. Her voice, soaring with arias of Bellini, Rossini, and Verdi — in tribute to Maria Callas — left us all spellbound.
Colleagues later described the experience with words such as:
- “We lived a dream…”
- “This is the definition of majesty.”
Joy and Robin’s Impressions
Months later, Jan McKenzie told me how her mother Joy had been so enchanted by Paros that she urged Robin to buy a small house on the island. And Robin himself, she recalled with a smile, declared that he felt “ten years younger” after their stay in Paros.
Epilogue
 I have shared only fragments of the story of the Paros Euromeeting — out of respect for Katerina, my Greek colleagues, and the truth of history.
I have shared only fragments of the story of the Paros Euromeeting — out of respect for Katerina, my Greek colleagues, and the truth of history.
One fact must be remembered: apart from accommodations with prices offered extremely cheap, every meal, every cultural and social event I have described was offered freely, as a gift of the Hellenic Institute — in the spirit of the noblest Greek hospitality.
Perhaps now it is clear why, in later years, whether in Crete for the 9th World Congress in 2005, or in Kos for the Euromeeting of 2019, our events were recognized perhaps, as the finest of their kind, both scientifically and organizationally.
With gratitude, George Spanos
ČJ
Paros Euromeeting 1998 – vzpomínky na nezapomenutelné setkání
George Spanos, Dip.MDT
V červnu 1998 hostil ostrov Paros Euromeeting McKenzie Institutu, který neměl období. Poprvé a naposledy naposledy dva dny. Magické kykladské prostředí, pečlivá organizace a řada překvapení vytvořily atmosféru, na kterou se dodnes vzpomíná. Největším unikátem byla samotná účast Robina a Joy McKenzie – v té době zcela bezprecedentní.
Tento příběh věnuji památce Robina McKenzie, profesora Apostolose Polyzoidise (průkopníka v oblasti kolenních protéz a poradců řeckých poboček) a mým drahým kolegům a přátelům, kteří vložili do organizace celé srdce. Zvláštní místo mají Sara Luetchford a Antoine Gemayel – jediní dva z tehdejších účastníků, kteří dosud neodešli do důchodu a stále aktivně působí.
Příjezd Robina a Joy
Jedno červnové ráno jsem spěchal svým malým Fiatem Uno Turbo na letiště Paros a obával se, zda se do něj vůbec vejde zavazadlo Robina a Joy. Když jsem dorazil, už jsem čekal venku, s úsměvem na tvářích.
„Připomínáme nám to Nový Zéland,“ řekli cestou do zátoky Naousa. Ostrov je okouzlil hned od prvního okamžiku.
Nečekaný pacient – dar od námořnictva
Osud zasáhl odpoledne. Kapitán torpédoborce HS Themistocles , zakotveného v zátoce Naousa, ležel už týden upoután na lůžko se značnou kořenovou bolestí do nohou a vybočením páteře. Po manuální korekci od George Spanose se jeho bolest zmírnila a trup se narovnal.
Uchvácen výsledek trval na tom, že se musí odvděčit. Druhý den pozval všechny účastníky Euromeetingu na palubu své lodi.
Téhož večera byli Robin a Joy McKenzie s kolegy z celé Evropy přivítáni s plnými vojenskými poctami řeckého námořnictva. Prohlédli jsme si radary, zbraně i kapitánský můstek, kde Robin usedl do kapitánského křesla. Večer vyvrcholil hostinou na moři – nezapomenutelným gestem řecké pohostinnosti.
Noci oslav
Oslavy pokračovaly tradiční kykladskou noc u hotelového bazénu: místní speciality, parské víno, hudba a tanec pod úplňkem. Přátelství se utužovala dlouho do noci.
Další den jsme navštívili starověké mramorové lomy v Marathi. Poté následovala přednáška profesora Polyzoidise o slavném parském mramoru – kameni, z něhož byla postavena Akropole i karyatidy Erechtheionu. Přednáška proběhla v historickém chrámu Panagia Ekatontapyliani, založeném v roce 237 nl a rozšířeném Justiniánem v 6. století.
Později jsme se prošli vesnicí Lefkes, kde kvetly bugenvileje a ibišky. Mezi mnoha zážitky vynikly dva: když jsme s Robinem společně zvonili na kostelní zvon a když Antoine Gemayel předpovídal Margaritě budoucnost z kávy v místní kavárně.
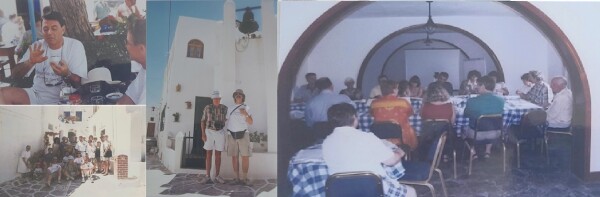
Soukromý koncert pod hvězdami
Večer nás profesor Polyzoidis pozval do své vily. Po slavnostní večeři zazpívala sopranistka Cathrin Monès árie Belliniho, Rossiniho a Verdiho – poctu Marii Callas, která všechny uchvátila.
Účastníci vzpomínají slovy:
- „Prožili jsme sen…“
- "Tohle je definice vznešenosti."
Odkaz na pohostinnost
O několik měsíců později mi Jan McKenzie řekl, že Joy byla Parosem tak okouzlena, že přemluvila Robina ke koupi domu na ostrově. A Robin prohlásil, že se po pobytu cítil „o deset let mladší“. Sdílím zde jen fragmenty příběhu Paros Euromeetingu — z úcty ke Kateřině, mým řeckým kolegům pokud pravděpodobnou historií. Jedno je však nutné připomenout: kromě ubytování nabízeného za velmi nízké ceny bylo každé jídlo, každou kulturní i společenská událost poskytnuta zdarma, jako dar řeckého institutu — ve znamení té nejvznešenější řecké pohostinnosti.
Nezapomenutelné zážitky z roku 1998 Paros Euromeeting 1998 zůstává jedinečný – nejen svou odbornou hodnotou, ale především srdečností, velkorysostí a nezapomenutelným duchem řecké pohostinnosti. Díky této tradici se McKenzie Institut vrátil do Řecka ještě dvakrát: na 9. světový kongres na Krétě v roce 2005 a na Euromeeting na Kosu v roce 2019 – obě akce patřily k nejlépe hodnoceným, vědecky i společensky.
S vděčností,
George Spanos
Sara Luetchford (Italy) – the bridge between London and Milan
 When Sara Luetchford graduated from Guy’s Hospital School of Physiotherapy in 1979, she could hardly have imagined that a few years later she would help shape the MDT landscape in Italy. Moving from England to Milan, she a entered a world of very basic physiotherapy. In the years ahead she introduced MDT to Italy, helped set up the first IFOMPT manual therapy master's course and many other manual therapy groups in Italy. Their search for methods of clear clinical logic made McKenzie courses a popular choice.
When Sara Luetchford graduated from Guy’s Hospital School of Physiotherapy in 1979, she could hardly have imagined that a few years later she would help shape the MDT landscape in Italy. Moving from England to Milan, she a entered a world of very basic physiotherapy. In the years ahead she introduced MDT to Italy, helped set up the first IFOMPT manual therapy master's course and many other manual therapy groups in Italy. Their search for methods of clear clinical logic made McKenzie courses a popular choice.
Sara brought with her the calm precision of British training and a sharp analytical mind. She earned her MDT Credentialing in 1992 and, just two years later, after obtaining the MDT Diploma in 1993, began teaching for the McKenzie Institute – first in Italy, then internationally. Today she directs the Altalena McKenzie Clinic in Milan, where she blends the disciplined reasoning of MDT with the quiet intuition of the experienced clinician.
Her path spans many qualifications in manual medicine, manual therapy and a masters in musculoskeletal rehabilitation, earning her OMPT membership, and collaboration on research into cervical and thoracic spine conditions. After three decades of teaching, her schedule remains full – including MDT courses across Europe, the Middle East and Asia. On the Mechanical Care Forum she once described how Italian physiotherapy transformed “before and after MDT” – patiently, without shortcuts, always through the patterns that patients reveal.
Her clinical signature remains constant: do a good assessment, find the treatment, give the patient the tool, and let the results speak for themselves.
Čj
Sara Luetchford (Itálie) – most mezi Londýnem a Milánem
 Když v roce 1979 Sara Luetchford dokončila fyzioterapii na Guy’s Hospital v Londýně, těžko mohla tušit, že o pár let později bude spolu-utvářet MDT scénu v Itálii. Z Anglie se přestěhovala do Milána, kde začala novou kapitolu života v zemi, kde fyzioterapie byla teprve v základním rozvoji systematického klinického myšlení. V následujících letech představila v Itálii koncept MDT, pomohla založit první magisterský program manuální terapie akreditovaný IFOMPT a stála u vzniku několika dalších odborných skupin zaměřených na manuální terapii. Hledání jasné klinické logiky tehdy vedlo mnoho terapeutů právě ke kurzům McKenzie.
Když v roce 1979 Sara Luetchford dokončila fyzioterapii na Guy’s Hospital v Londýně, těžko mohla tušit, že o pár let později bude spolu-utvářet MDT scénu v Itálii. Z Anglie se přestěhovala do Milána, kde začala novou kapitolu života v zemi, kde fyzioterapie byla teprve v základním rozvoji systematického klinického myšlení. V následujících letech představila v Itálii koncept MDT, pomohla založit první magisterský program manuální terapie akreditovaný IFOMPT a stála u vzniku několika dalších odborných skupin zaměřených na manuální terapii. Hledání jasné klinické logiky tehdy vedlo mnoho terapeutů právě ke kurzům McKenzie.
Sara přinesla do Itálie britskou preciznost, klid a analytický přístup. V roce 1992 složila akreditační zkoušku v Mechanické diagnostice a terapii (MDT) a už o dva roky později, po dokončení diplomovaného studia v MDT v roce 1993, předávala své zkušenosti jako instruktorka McKenzie Institute – nejprve doma v Itálii, později i mezinárodně. Dnes vede Altalena McKenzie Clinic v Miláně, kde propojuje systematické myšlení MDT s citlivým klinickým úsudkem typickým pro „starou školu“ britské fyzioterapie.
Její profesní cesta je pestrá – od manuální medicíny a manuální terapie, magisterský titul z muskuloskeletální rehabilitace a členství OMPT až po spolupráci na výzkumech krční a hrudní páteře. Přestože učí přes tři dekády, její rozvrh je stále nabitý – vyučuje MDT kurzy po celé Evropě, na Blízkém východě i v Asii. V rozhovoru pro Mechanical Care Forum výstižně popsala, jak se italská fyzioterapie proměnila „před a po MDT“ – trpělivě, bez zkratek, s respektem ke klinickým vzorcům, které ukazují sami pacienti.
Její klinický rukopis zůstává stejný: udělej dobré vyšetření, najdi léčbu, dej pacientovi nástroj a nech výsledky mluvit za sebe.
Helen Clare (Australia) – the voice that gave MDT its global face
 When Helen Clare graduated from the University of Otago in 1975, she could hardly have imagined that she would spend the majority of her professional life involved with the McKenzie Institute. After several years of clinical practice, she moved to Sydney, to take the opportunity of postgraduate studies. She completed a post graduate Diploma in Manipulative Therapy which stimulated be interest in the McKenzie Method of treating musculo-skeletal disorders. She reached out to Robin McKenzie in 1986 and was appointed as one of his panel of Instructors later that year.
When Helen Clare graduated from the University of Otago in 1975, she could hardly have imagined that she would spend the majority of her professional life involved with the McKenzie Institute. After several years of clinical practice, she moved to Sydney, to take the opportunity of postgraduate studies. She completed a post graduate Diploma in Manipulative Therapy which stimulated be interest in the McKenzie Method of treating musculo-skeletal disorders. She reached out to Robin McKenzie in 1986 and was appointed as one of his panel of Instructors later that year.
In the late 1980s, she was among the first to systematically evaluate the effectiveness of the McKenzie Method – first in practice, later through research. Her PhD thesis Evaluation of the McKenzie Method added to the growing research evidence on Mechanical Diagnosis and Therapy ( MDT)
In 1989 she had joined the International faculty of the McKenzie Institute and in 1999 became its Director of Education working closely with Robin Mckenzie . Under her leadership, the MDT educational program was standardised worldwide. It has been taught in over fifty countries and has become an established part of post-graduate physiotherapy education worldwide.
In 2018 Helen took on a different very different role in the McKenzie Institute International. She was appointed CEO and has focused since then on communication and unity within the Institute and supporting the Institute’s vision of ensuring those experiencing musculoskeletal disorders will have access to the highest quality care by clinicians trained and certified in the McKenzie Method of Mechanical Diagnosis and Therapy.
Helen is profoundly aware of the story behind every patient and every clinician. She strives to achieve the best outcome for both. She feels a responsibility to grow Robin McKenzie’s legacy through the delivery of high-quality education in MDT for clinicians worldwide.
ČJ
Helen Clare (Austrálie) – hlas, který dal MDT globální tvář
Když Helen Clare v roce 1975 absolvovala studium fyzioterapie na University of Otago, sotva mohla tušit, že většinu svého profesního života zasvětí práci pro McKenzie Institut. Po několika letech klinické praxe se přestěhovala do Sydney, aby využila příležitost k postgraduálnímu studiu. Získala postgraduální diplom z manipulační terapie, který v ní probudil zájem o McKenzieho metodu léčby muskuloskeletálních poruch. V roce 1986 se spojila s Robinem McKenziem a ještě téhož roku byla jmenována členkou jeho instruktorského týmu.
Na konci 80. let patřila mezi první odborníky, kteří začali systematicky hodnotit účinnost McKenzie metody – nejprve v klinické praxi, později i výzkumně. Její doktorská práce Evaluation of the McKenzie Method významně přispěla k rostoucí vědecké základně metody mechanické diagnostiky a terapie (MDT).
V roce 1989 se stala členkou mezinárodní lektorské fakulty McKenzie Institute a v roce 1999 převzala funkci ředitelky vzdělávání, v úzké spolupráci s Robinem McKenziem. Pod jejím vedením byl vzdělávací program MDT sjednocen a standardizován po celém světě. Dnes se vyučuje ve více než padesáti zemích a stal se nedílnou součástí postgraduálního vzdělávání fyzioterapeutů.
V roce 2018 přijala Helen zcela novou roli v McKenzie Institute International – byla jmenována výkonnou ředitelkou (CEO). Od té doby se soustředí především na komunikaci a sjednocení v rámci institutu a na podporu jeho vize: zajistit, aby lidé s muskuloskeletálními poruchami měli přístup k nejkvalitnější péči poskytované terapeuty vyškolenými a certifikovanými v McKenzieho metodě mechanické diagnostiky a terapie.
Helen si hluboce uvědomuje příběh, který stojí za každým pacientem i za každým terapeutem. Usiluje o to, aby výsledek byl co nejlepší pro oba. Cítí odpovědnost rozvíjet odkaz Robina McKenzieho prostřednictvím poskytování vysoce kvalitního vzdělávání v MDT terapeutům po celém světě.
Antoine Gemayel – the bridge between Rome and Beirut who carried MDT across continents When Antoine Gemayel was leading physiotherapy services in Rome in the late 1980s, he could hardly have imagined that he would become one of the key figures responsible for spreading MDT from Europe to the Middle East. Born in Lebanon and professionally shaped in Italy, he built a genuine bridge between two worlds — the Mediterranean clinical tradition and the rapidly developing physiotherapy landscape of the Levant.
When Antoine Gemayel was leading physiotherapy services in Rome in the late 1980s, he could hardly have imagined that he would become one of the key figures responsible for spreading MDT from Europe to the Middle East. Born in Lebanon and professionally shaped in Italy, he built a genuine bridge between two worlds — the Mediterranean clinical tradition and the rapidly developing physiotherapy landscape of the Levant.
In 1990, he founded the McKenzie Institute – Italia, leading it until 2014. He was among the first to introduce MDT in a structured way into a country with a long-established manual therapy tradition, helping to create clear educational pathways and clinical standards.
From 1998 to 2009, he served on the Advisory Council of the McKenzie Institute International, and since 2019 he has led the McKenzie Institute Lebanon and Middle East, which he also founded.
His professional journey reflects the two cities where he has spent most of his life:
– since 1997, he has run private practices in Rome and Beirut,
– from 1989 to 1997, he served as Head Physiotherapist at Associazione Laziale Motulesi in Rome,
– between 1971 and 1989, he led physiotherapy services at Associazione Anni Verdi.
His education spans more than five decades:
a Lebanese PT diploma (1969), an Italian PT diploma (1997), Vojta training (1977–1978), Sophie Levitt’s cerebral palsy course (London, 1970), and manual therapy qualifications under Prof. Marcel Bienfait (1986–1987).
He completed MDT Courses A–D in the late 1980s, passed his Credentialing Exam in 1995, and earned his Diploma in MDT in 1997 in the USA.
His teaching footprint is equally extensive:
– since 2000, he has been Senior Faculty of the Italian Branch,
– since 2005, an International Faculty member teaching MDT Courses A–E,
– from 2005 to 2015, he taught extensively across France, supporting Gabor Szigeti in developing the branch and forming new instructors,
– in addition to Italy, France and Lebanon, he has taught MDT courses in Egypt, Jordan and Saudi Arabia.
His linguistic skills mirror his international reach: native Arabic and fluent French, English and Italian — the three languages in which he regularly teaches MDT.
For his long-standing contribution to MDT, he received the Extension Award in 2013.
Antoine Gemayel is not only an MDT educator — he is one of the rare individuals who helped the method take deep root in two regions he calls home: Italy and Lebanon. His work connects cultures, systems and ways of thinking, showing how MDT can travel far beyond national borders.
ČJ
Antoine Gemayel – most mezi Římem a Bejrútem, který přenesl MDT mezi kontinenty
Když Antoine Gemayel koncem 80. let vedl fyzioterapii v Římě, netušil, že se o několik desetiletí později stane jednou z nejvýraznějších postav, které přenesou MDT z Evropy až na Blízký východ. Původem z Libanonu, profesně formovaný v Itálii, vybudoval most mezi dvěma světy – mezi středozemní klinickou tradicí a rychle se rozvíjející fyzioterapií Levantu.
V roce 1990 založil McKenzie Institute – Italia a až do roku 2014 jej vedl. Byl jedním z těch, kteří do země s bohatou tradicí manuální terapie přinesli MDT v systematické podobě a pomohl vytvořit jasnou vzdělávací strukturu i klinické standardy.
V letech 1998–2009 působil v Advisory Council McKenzie Institute International a od roku 2019 vede pobočku McKenzie Institute Lebanon and Middle East, kterou rovněž založil.
Jeho profesní cesta odráží dvě města, v nichž strávil většinu života:
– od 1997 provozuje soukromé praxe v Římě a Bejrútu,
– v letech 1989–1997 byl hlavním fyzioterapeutem v Associazione Laziale Motulesi v Římě,
– mezi 1971–1989 vedl fyzioterapii v Associazione Anni Verdi.
Jeho vzdělání pokrývá více než pět dekád praxe:
libanonský diplom fyzioterapeuta (1969), italský PT diplom (1997), Vojtova metoda (1977–1978), kurz Sophie Levitt (Londýn, 1970), manuální terapie pod vedením Marcela Bienfaita (1986–1987).
K MDT se dostal již koncem 80. let — absolvoval kurzy A–D, v roce 1995 složil Credentialing a v roce 1997 získal Diploma MDT v USA.
Jeho výuková činnost je široká:
– od roku 2000 je Senior Faculty McKenzie Institute Italia,
– od roku 2005 člen International Faculty, vyučuje kurzy A–E po celém světě,
– v letech 2005–2015 vyučoval intenzivně ve Francii, kde pomáhal Gáboru Szigetimu formovat novou generaci francouzských instruktorů a rozvíjet tamní pobočku,
– kromě Itálie a Francie učil kurzy také v Egyptě, Jordánsku a Saúdské Arábii.
Jazykově je stejně mezinárodní jako jeho profesní působení: rodná arabština, plynulá francouzština, angličtina a italština. Právě angličtinu, francouzštinu a italštinu používá při výuce MDT.
Za dlouholetý přínos MDT obdržel v roce 2013 prestižní Extension Award.
Antoine Gemayel není jen lektorem MDT — je jedním z těch, kteří pomohli metodu zakořenit v regionech, které tvoří jeho domov: v Itálii i v Libanonu. Jeho práce propojuje kultury, systémy i myšlení a ukazuje, jak MDT může přesáhnout hranice jednotlivých zemí.
Stacey A.Lyon – the heart and driving force of the McKenzie Institute USA
 When Stacey Lyon joined the McKenzie Institute USA in 1995, she stepped into a world where physiotherapy was evolving rapidly and MDT was beginning to take shape as a structured educational system. She was not a clinician — yet she became one of the most influential people behind the growth and stability of MDT in the United States.
When Stacey Lyon joined the McKenzie Institute USA in 1995, she stepped into a world where physiotherapy was evolving rapidly and MDT was beginning to take shape as a structured educational system. She was not a clinician — yet she became one of the most influential people behind the growth and stability of MDT in the United States.
Stacey soon became the Executive Director of the U.S. branch and has served on its Board of Directors since 1998. Much of her work happens behind the scenes, but without her, the USA branch and faculty, MDT educational programming, administrative support and nationwide coordination simply would not function as smoothly as they do.
In 2015, she was appointed to the Strategic Council of the McKenzie Institute International — the platform where the global vision of MDT is shaped and works closely with the MII Board of Trustees. Her ability to connect people, systems and countries has been crucial for building the strong organisational foundation that MDT enjoys today in the U.S. and internationally.
Stacey received the Institute’s International Extension Award in 2018, given to individuals whose long-standing contributions have significantly shaped the McKenzie Institute and MDT community.
She is widely regarded as the “quiet driving force” of McKenzie Institute USA — the person behind every well-run course, every seamless communication chain, every strategic decision that keeps MDT moving forward. Her contribution is different from that of clinicians, but essential: MDT stands on strong foundations largely because of her.
ČJ
Stacey A. Lyon – srdce a motor McKenzie Institute USA
Když se Stacey Lyon v roce 1995 připojila k McKenzie Institute USA, vstoupila do prostředí, kde se fyzioterapie rychle vyvíjela a MDT začínala získávat podobu strukturovaného vzdělávacího systému. Nebyla klinikem — a přesto se stala jednou z nejvlivnějších osobností stojících za růstem a stabilitou MDT ve Spojených státech.
Stacey se brzy stala výkonnou ředitelkou americké pobočky a od roku 1998 působí v její správní radě. Velká část její práce probíhá „v zákulisí“, ale bez ní by americká pobočka, její fakultní tým, vzdělávací programy MDT, administrativní podpora i celonárodní koordinace rozhodně nefungovaly tak hladce, jak je tomu dnes.
V roce 2015 byla jmenována do Strategické rady McKenzie Institute International — platformy, kde se formuje globální vize MDT — a úzce spolupracuje s mezinárodní správní radou MII. Její schopnost propojovat lidi, systémy a země byla klíčová pro vybudování silných organizačních základů, na kterých MDT stojí v USA i mezinárodně.
V roce 2018 obdržela Mezinárodní cenu Extension Award, udělovanou osobnostem, jejichž dlouhodobý přínos významně formoval McKenzie Institute a MDT komunitu.
Je široce vnímána jako „tichá hybná síla“ McKenzie Institute USA — osoba stojící za každým dobře zorganizovaným kurzem, každým bezchybným komunikačním řetězcem a každým strategickým rozhodnutím, které posouvá MDT kupředu. Její přínos je jiný než přínos kliniků, ale stejně zásadní: MDT stojí na pevných základech z velké části díky ní.
Scott Herbowy — a quiet powerhouse of MDT in America
 When Scott Herbowy began his journey in physical therapy, few could have predicted how profoundly he would shape the story of MDT in the United States. His path is not the loud or self-promoting kind — it’s the steady, disciplined, quietly transformative path of someone who shows up, teaches, listens, and builds something that lasts.
When Scott Herbowy began his journey in physical therapy, few could have predicted how profoundly he would shape the story of MDT in the United States. His path is not the loud or self-promoting kind — it’s the steady, disciplined, quietly transformative path of someone who shows up, teaches, listens, and builds something that lasts.
Scott earned his Diploma in Mechanical Diagnosis and Therapy (Dip. MDT) in September 1992 — at a time when MDT in the U.S. was still finding its direction. Just a year later, he joined the Institute’s teaching faculty as a Junior Instructor, and by 2001 he was Senior Faculty, guiding generations of clinicians with precision, calmness and an exceptional command of clinical reasoning.
Alongside his teaching, Scott built decades of experience as an Orthopaedic Clinical Specialist (OCS), treating real patients with real problems — the kind of work that deepens intuition and sharpens judgment. This combination of clinical depth and educational clarity became his signature as a mentor and instructor.
Over the years, he has delivered hundreds of MDT courses across the United States and internationally, shaping not only how MDT is taught, but how it is understood. He was among the first instructors to lead extremity-focused MDT courses, helping to expand the method far beyond its traditional spinal roots.
And one fact speaks volumes about his lasting influence:
he has spent more than 16 years as a Diploma Clinical Instructor — and has helped train and mentor over 20 clinicians who are now part of the MDT teaching faculty worldwide.
This alone places him among the most impactful educators in the history of MDT.
Today Scott runs his private practice in Austin, Texas, where he blends patient care with teaching and mentorship. Those who have learned from him often describe the same experience: a teacher who makes complexity understandable, who gives confidence rather than pressure, who helps clinicians find their own clinical voice.
Why he matters:
Scott is not the kind of clinician who merely follows standards — he is someone who strengthens them, refines them, and hands them on. Through decades of thoughtful teaching, mentorship, and clinical practice, he has become one of the pillars on which the MDT community in the United States stands.
ČJ
více než 16 let působil jako diploma clinical instructor a pomohl vychovat přes 20 terapeutů, kteří dnes tvoří MDT výukovou fakultu po celém světě.
Scott není terapeut, který by pouze následoval standardy. Je to ten, kdo je upevňuje, rozvíjí a předává dál. Díky desetiletím výuky, mentorování a klinické práce je dnes jedním z pilířů MDT komunity v USA.
Kathleen (Kathy) Hoyt (USA) – the woman who opened the door to MDT in America
 Kathy Hoyt graduated Physical Therapy Training from Columbia University, NY in 1974. Her first position was at Rancho Los Amigos Hospital, a premier Rehabilitation and research center in California. There she had the opportunity to work with Vert Mooney MD who was an Orthopedic surgeon who was driven to understand patient's pain and how it effected function. He was also very supportive of cutting edge physical therapy. Kathy had the opportunity to meet and learn from many orthopedic manual therapists ,including Robin McKenzie. Kathy completed an Orthopedic Physical Therapy Residency program at Kaiser Permanente where she learned and applied various Manual Therapy approaches, but felt that the McKenzie Method provided the best framework for clinical practice and measurable positive patient outcomes.
Kathy Hoyt graduated Physical Therapy Training from Columbia University, NY in 1974. Her first position was at Rancho Los Amigos Hospital, a premier Rehabilitation and research center in California. There she had the opportunity to work with Vert Mooney MD who was an Orthopedic surgeon who was driven to understand patient's pain and how it effected function. He was also very supportive of cutting edge physical therapy. Kathy had the opportunity to meet and learn from many orthopedic manual therapists ,including Robin McKenzie. Kathy completed an Orthopedic Physical Therapy Residency program at Kaiser Permanente where she learned and applied various Manual Therapy approaches, but felt that the McKenzie Method provided the best framework for clinical practice and measurable positive patient outcomes.
In 1977 she helped organize the very first McKenzie course in California, United States – a small step that sparked a nationwide movement. Over the years, she became one of the most influential figures in the American MDT community – a clinician, teacher, leader and mentor.
As the founding Chair of the McKenzie Institute USA, she along with other faculty, built the educational framework that continues to support therapists across the country. She was also instrumental in developing the MDT Residency and Fellowship programs – and in shaping the idea that MDT is not just a technique, but a way of thinking clinically.
Kathy Hoyt often reminds us that the real power of MDT does not lie in the therapist’s hands but in the clinician's clinical reasoning and the patient’s ability to understand and influence their own healing. Her story is one of vision and courage – of someone who started before there was a path, and helped pave one for the rest of us.